Can We Validate Anecdotal Data? Measuring What Firefighters Think They Know
Key Takeaways
- Anecdotal data, or data that are collected in a nonsystematic way that’s reliant on personal stories from firefighters, may serve as a tool to elaborate on identified issues but also might lead fire service managers to draw incorrect conclusions and contribute to wasting resources and inefficiency.
- Fire department data analysts might not be on a rig every day, but they play a critical role in ensuring that the department and other public safety stakeholders perceive risk correctly and put the right tools on the right problems.
- A coalition of municipal stakeholders, such as the fire department, private ambulance services, homeless shelters, housing authories and local healthcare systems, that uses fire department response data can improve the quality of ilfe for residents, visitors and fire department members.

When new fire investigators go through their initial training, adherence to the scientific method is emphasized repeatedly. Another way to describe application of the scientific method is that investigators objectively must follow where the observed data lead them.
The same principle applies in the newer field of fire service data analysis. The days of relying solely on anecdotal reporting from crews in one’s operations division are long over. Furthermore, when departments speak to hazards and risks and their level of activity in particular neighborhoods or their jurisdiction as a whole, they must be able to communicate with confidence about clean, validated data. Anecdotal data, or data that are collected in a nonsystematic way that’s reliant on personal stories from firefighters, may serve as a tool to elaborate on identified issues but also might lead fire service managers to draw incorrect conclusions and, ultimately, contribute to wasting resources and inefficiency.
Fire department data analysts might not be on a rig every day, but they play a critical role in ensuring that the department and other public safety stakeholders perceive risk correctly and put the right tools on the right problems.

Assumptions vs. insights
The downtown area of Champaign, IL, is the social, cultural and economic heart of the city. For these reasons, city government has a vested interest in ensuring the health and vibrancy of the core area.
I was tasked with looking at 25 months (July 1, 2023–July 31, 2025) of fire department response data as part of a project to assess the overall level of safety in downtown. Owing to recent instances of violent crime and economic uncertainties, there’s been a perception that downtown no longer is a safe place for people to work, dine and seek entertainment. That perception is at least partly held by Champaign Fire Department (CFD) crews who work at the department’s headquarters station at the lower edge of the downtown area, who assert that they “always” see certain types of calls at certain addresses. Analysis of incident reports challenged many of their assumptions and yielded valuable insights on how the frequency and severity of emergency calls for service in this area of the jurisdiction could be reduced—the core goal of any community risk reduction (CRR) initiative.

Analysis of call volume
During the measurement period, the CFD responded to 19,972 calls for service. Of those, 2,298 occurred in the downtown area and constituted 11.5 percent of the total call volume.
Incidence of fire calls track with historic averages that are noted in the city’s 2023 Community Risk Assessment (CRA), which is about 2 percent of total call volume. However, from July 2023–December 2024, the CFD responded to 15 percent more medical calls in the downtown area compared with other station areas throughout the city. From January 2025–July 2025, the department responded to medical calls downtown at a rate that was 20 percent higher than that of the other areas of the city. None of the companies that worked in this area of the city commented on incidence of motor vehicle accidents (MVAs), but the number of MVAs is believed to be greater than it should be, given that walking and cycling are encouraged in this area. Distribution of calls was consistent, with higher call volume noted in warmer months and lower call volume in colder months.
Firefighters consistently report that they believe that the downtown area is busier on weekends, and records indicate that Friday and Saturday are the busiest days of the week. However, the call volume on Wednesday and Thursday is only slightly less than that of the peak times. These data prompted us to examine not only when the calls happen in this part of the city but where they occur.
Frequent utilizers
Every jurisdiction has certain addresses that are frequent utilizers of emergency services—and are the subject of firefighter complaints. As a professional body, the department tends to look at all of its calls for service through the lens of a fire event (i.e., there’s a fire in a building, we come to put it out, the building usually doesn’t suffer another fire, on to the next event).
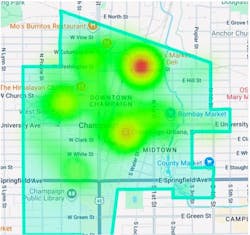
In the context of medical emergencies and invalid assist calls, though, this isn’t a perspective that encourages definitive solutions. If Joe and Jane Firefighter want to stop going to those high-frequency 3 a.m. calls, department analysts must do some more digging into their response data. In the CFD’s case, the data revealed that most of the department’s calls in the downtown area came from four addresses.
The most frequently visited address is a low-barrier shelter for people who are experiencing homelessness. The second-busiest is a bus and train station. The third-busiest address is an assisted-living facility for people with developmental disabilities. The fourth address is a mid-rise apartment building that’s operated by the Housing Authority of Champaign County.
For the two busiest downtown addresses, the department found that the majority of its patients used 9-1-1 as their entry into the healthcare system for mental health emergencies, substance abuse and withdrawal systems, and sudden onset respiratory difficulty. There also are more calls for trauma to these addresses than for others in the examined area.
For calls to the low-barrier shelter, the department found that slightly more than one-third of the time, it responded back within 2½ hours for another medical call. This at least partially validates the anecdotal reporting of CFD crews who believe there is a “waterfall effect” once they respond to this address for the first time in a shift.
Conversely, the issues that were encountered by residents at the latter two addresses were slightly different. Although the addresses also are a socioeconomically stressed population group, these calls mostly were related to difficulties in managing chronic health conditions, such as chest pain, diabetes and high blood pressure.
Given that one of the addresses is a type of care facility and the other is managed by a government agency, there are opportunities to build educational partnerships, giving residents the tools that they need to live healthier lives and to manage the ongoing conditions for which they often call 9-1-1. Interestingly, for CFD crews’ reporting of “frequent fliers,” neither of these addresses came up during conversation, and many downtown firefighters were surprised at how often they responded to these buildings.
Multiple benefits
This project started with the question of whether this part of our city is safe for residents who frequent the downtown area. Looking at 25 months of recent response data from the fire department perspective, it doesn’t appear that downtown is more or less dangerous than other parts of the city. However, in keeping with the principle that we must follow where the data lead us, we generated insights that will help to better serve residents who utilize fire department services the most often, while confirming some assumptions that are held by CFD firefighters and disproving others.
Certainly, high-frequency and low-acuity medical calls for service aren’t solved definitively by dispatching a pumper and an ambulance. People who experience homelessness need mental health and other healthcare resources that give them the tools to prevent a health problem from turning into an emergency. Socioeconomically stressed residents who have chronic health conditions should have a mobile integrated health resource that mitigates conditions that can lead to medical emergencies. This preventative infrastructure—CRR geared toward reducing medical calls—currently doesn’t exist in the community and requires a coalition of varied stakeholders, such as:
- Champaign Fire Department
- Private ambulance services
- City of Champaign Township (manages shelter)
- Housing Authority of Champaign County
- Local healthcare systems
Such a coalition will improve quality of life for city residents that the department serves the most often while reducing the frequency and severity of fire department emergency calls for service. Altering response to the needs of these residents is a CRR goal that benefits everyone who’s involved and, tying back to the original objective, creates a better environment downtown for everyone.
Lastly, pertaining to how firefighters view their calls for service, it gives the fire department and partner agencies the best chance to make sure that a solved problem stays solved. Their anecdotal data told part of the story, but it takes street firefighters and fire department analysts who work together to generate insights and maximize service delivery.
About the Author

Jeremy Mitchell
A 25-year veteran of the fire and EMS services, Jeremy Mitchell serves as deputy fire marshal of the Champaign, IL, Fire Department. He also serves on the Technical Committees for NFPA 1030: Standard for Professional Qualifications for Fire Prevention Program Positions and NFPA 1300: Standard on Community Risk Assessment and Community Risk Reduction Plan Development and is a founding member of the Association of Fire and Emergency Services Analysts.